Bringing Protocols to Life to Reduce Site and Patient Burdens
In a world where clinical trials are growing larger and protocols more complex, it’s increasingly important that study sponsors make sure to get their protocols right from the start to avoid unwanted delays or cost overruns due to mistakes, deviations or even just failure to correctly forecast the time, money and resources needed to conduct a study.
And that means that the art and practice of protocol optimization, utilizing input not only from target patient groups, but from potential site partners, as well, becomes ever-more important.
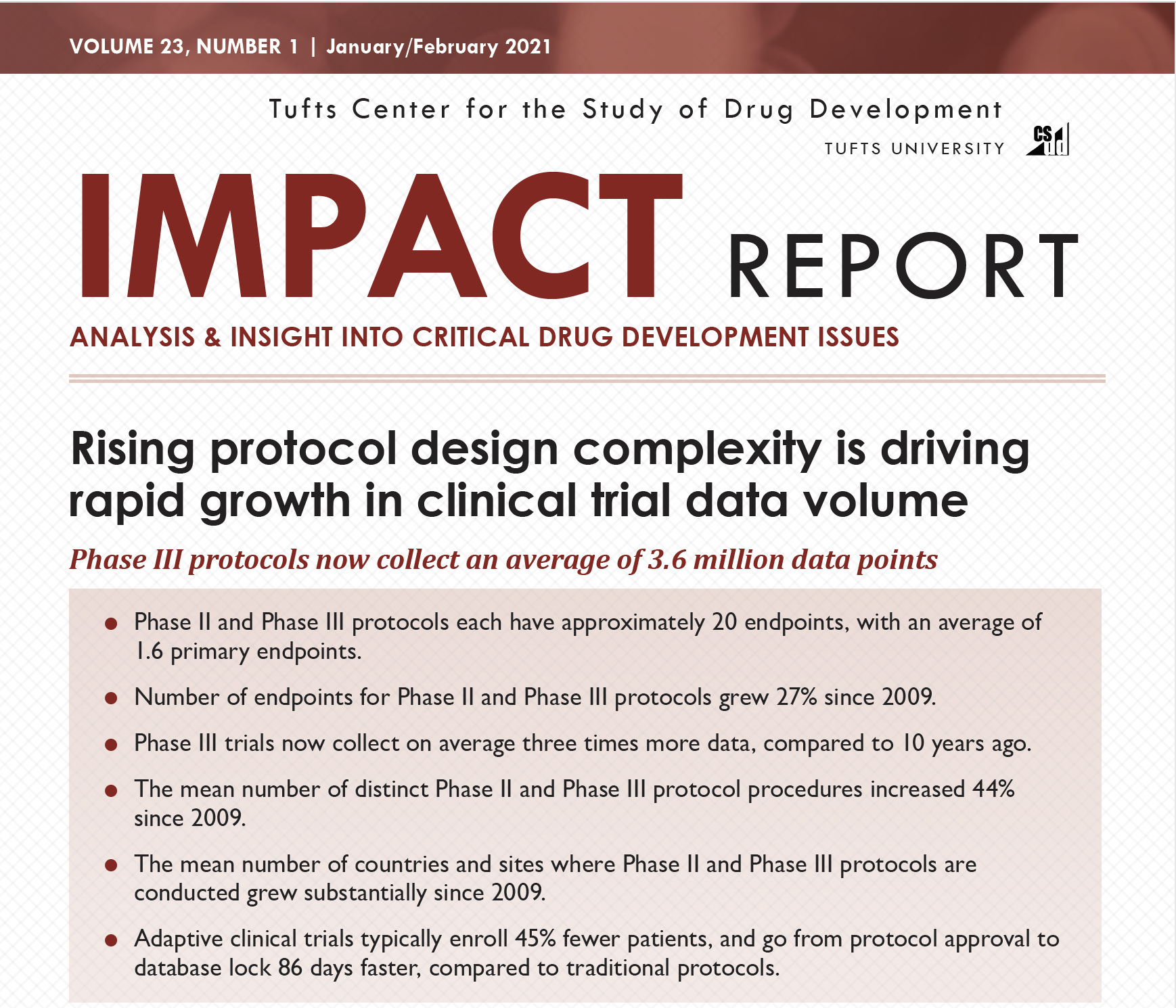
Protocols are getting more complex for many reasons, such as regulatory demands, expansion into more challenging indications like rare disease and immunology, adaptive study designs and trying to get as much data from one study as possible. A 2021 study by the Tufts Center for the Study of Drug Development (CSDD) noted that protocols have been growing increasingly complex since 2009, with no end in sight to that trend. For instance, the CSDD report said that Phase II and III protocols as of 2020 generally had about 20 endpoints, with an average of 1.6 primary endpoints, up 27% since 2009. And the mean number of distinct procedures required for a typical protocol rose 44% during the same timeframe.
Amendments are also increasing. CSDD noted in an early 2022 report that the mean number of protocol deviations and substantial amendments—another cost and time driver—have increased across all clinical trial phases. The typical Phase 3 trial has 119 deviations, the CSDD report said. More amendments mean more operational burdens for sites, longer cycle times and more chances for deviations.
And about 30% of patients in Phase 2 and 3 studies have deviations; more deviations can lead to poorer quality data and outcomes. But many amendments, as well as deviations, can be avoided by better planning up front, especially in the face of more complex protocol designs.
Feasibility should be a conversation
Protocols typically are written to meet regulatory obligations, not to help research sites efficiently operationalize them. This leads to a disconnect when it comes to operational feasibility. At most, sites will check off a feasibility form that indicates whether they do or do not have particular equipment and access to desired patients.
But operational feasibility needs to be viewed as more of a process or a conversation, not just completion of a simple form. And protocol optimization is the means by which operational feasibility can be built into the study design from ground zero.
Protocol optimization can be viewed as an in-depth examination of the who, what, where, when, why and how of what it will take to conduct a successful clinical trial. In most cases, protocols do a good job of explaining what must happen when—in other words, detailing the procedures to be followed and the schedule. But questions often arise around the who and the how of protocol implementation.
The who is generally viewed as the target patient population. The protocol must define this group very clearly, explaining how the patients are characterized and defining specific inclusion and exclusion criteria.
Sponsors generally do a good job of defining the patient population they want to target with different clinical trials. However, the way they communicate this information in the protocol is rarely optimal. For example, most protocols include numerous inclusion and exclusion criteria, but provide them in a random order. Some may be copied from previous protocols or from a corporate template. But rarely are the criteria written with consideration of, for instance, how sites will go through potential patients’ medical records.
A better approach would be to provide some sort of organization of the criteria that aligns well with normal site workflow. For instance, inclusion/exclusion criteria could be organized by body systems, medications used or time restrictions, among other categories.
This sort of enrollment optimization can make the protocol more easily understandable—and thus, easier to execute correctly—for both patients and research sites. And that means fewer enrollment issues and reduced chance of deviations related to patient recruitment, enrollment and informed consent.
A site-centric approach to better explain the ‘how’
The other area in which protocols tend to need optimization is in explaining exactly how, in sufficient detail, protocol activities are to happen. And this is an area where early input from target sites themselves can be invaluable.
Patient-centricity has become a buzzword within the clinical research industry, with sponsors, sites and even regulators emphasizing the importance of providing a positive patient experience to aid in recruitment and retention of study participants. This can include factors like schedule flexibility and use of decentralized features or technology to increase convenience for patients.
In order for that to happen, patient-centricity must be built into a protocol from its inception, using real-life input from patients and advocates about the real needs and preferences of the target population, as Mike Lang noted in a blog post on the Pro-ficiency website. And that means that protocols need to be optimized with an eye toward real-life patient needs and preferences, usually by getting input from patient groups during the protocol design stage.
But patient centricity can be difficult to achieve if sites are not fully capable of delivering an optimum experience. What is often missing is a site-centric approach to determining what is truly feasible, as well as what time, equipment and human resources are realistically needed for a protocol to be viable. In some ways, the emphasis on patient-centricity has led to less consideration of operational feedback from sites.
And in reality, one of the most patient-centric actions sponsors can take is taking a site-centric approach to optimizing their protocols. Sites interact with patients and are responsible for implementing protocols in a patient-centric way, so making the protocol more organizationally feasible for sites will ultimately add to patients’ experiences.
And this type of information can only come with early feedback from sites. If protocols are not absolutely clear on the ‘how’ of implementation, down to the smallest detail, that leaves sites with room for interpretation based on their individual capabilities, set-ups and standard practices. The end result? In essence, a study could have 200 sites around the world applying their own interpretations to protocols. This can lead to cost overruns due to under-estimating staff or equipment needs, or protocol deviations or mistakes due to unplanned glitches in operations.
For instance, protocols often use footnotes or separate operational manuals to provide precise instructions on how to carry out various activities. A protocol may state that sites need to take patients’ blood pressure at visits on a certain schedule. And sites may take this information to estimate the time needed for each visit, as well as estimating the associated person-hours that must be funded. But if a footnote or manual then mandates that the measurement be taken standing for a certain amount of time and sitting for a certain amount of time, this can throw off the estimated visit time needed and drive up time and costs.
Similarly, a protocol may mention pharmacokinetic sampling requirements at certain visits. But the supplemental information might stipulate widely different timing relative to the study drug dose at different visits.
Even facility layout can pose a challenge, if the pharmacy is supposed to prepare a sensitive treatment within a certain timeframe but the distance from the pharmacy to the clinic is too far to allow that timeline to be met.
This can be further complicated if there are errors or inconsistencies in any of the supporting documents or footnotes. And that issue is exacerbated by the need to maintain version control and accuracy of all these parts if one is updated.
Visualizations help bring the protocol to life for sites
But sponsors can work with sites to avoid many of these problems and prevent confusion that can lead to errors, deviations and delays. It comes down to operational feasibility. Factors that are most important to sites are those that involve what they must do, when they must do it and how they must do it.
It’s not enough for a site to check off that it has access to patients or certain equipment or facilities. These basic qualifications may not tell the whole story of how easy or difficult a protocol may be for a given site to implement. For instance, a site may have broad access to diabetes patients, but may not have many that meet all 70 inclusion criteria listed in a particular protocol.
Sponsors cannot provide this information to sites unless they look at the protocol through the lens of the staff that must implement it. And in order to do this, it’s important for sponsors to get complete and accurate evaluations from sites so that the protocol writers can incorporate that feedback into the finished protocol. Not all sites are structured the same, so some consideration may be required for variation among sites that they want to include in a study.
All parties must fully understand the study design and timeline so that they can see clearly how complex it will be in real life. It may be helpful for some sponsors to work with outside protocol optimization experts to ensure that they cover all their bases from the inception of each study protocol. Pro-ficiency’s proprietary optimization methodology, Pro-Active Protocol, can help achieve that goal by applying simulation to visually represent the operational flow of a clinical study.
For instance, visual mapping can be done to show, step-by-step, how drug preparation must be conducted, rather than forcing sites to figure out how to implement that part of the protocol without having to piece together information from multiple documents. Sites can then see clearly how those steps would work within their own organizational structures.


This ability to help sponsors and sites visualize the information contained in disparate documents is a key value of services like Pro-Active Protocol.
In this way, sponsors and sites can experience a “day in the life” of a planned study, looking at it from both a site organizational and patient experience view. This insight will prove invaluable. Not only will it allow sponsors to incorporate feedback from sites and patients into the protocol design, but the simulation can be used later to let sites and patients understand in mere minutes exactly what participation in a study will entail, including possible curve balls like patient relapse.
This can aid enrollment by letting patients understand viscerally how study participation will fit into their lives. And it can aid in site selection, preparation and training by giving sites a clear view of what study participation will demand of their organizational structures and procedures.
Get in touch to learn more: http://proficiency1.wpenginepowered.com/contact-us/

Beth Harper, Chief Learning Officer at Pro-ficiency, is on a mission to eliminate protocol deviations. Beth brings 35-plus years of experience in clinical research operations to Pro-ficiency, utilizing this knowledge along with her years of creating live protocol simulation training to create cutting-edge simulation training programs at Pro-ficiency. Beth has published and presented extensively in the areas of study feasibility, site selection, patient recruitment, protocol optimization, sponsor/site relationship management and clinical research professional competencies. Beth received her B. S. in Occupational Therapy from the University of Wisconsin and an M.B.A. from the University of Texas.
{kind=link}
{kind=link}