An approach to training that carefully targets site and individual weak areas, along with critical protocol procedures, could not only reduce deviations, but can play a key role in reducing overall burdens on research site personnel.
Booming administrative tasks, customized technology systems and redundant certification and training requirements are among the primary factors that clinical research staff say eats up time better spent with patients and adds excessive burden—often uncompensated—to study teams. Some of these developments have been laid at the feet of growing protocol complexity and trial sizes, which are likely problems that are here to stay. But others lie within sponsors’ capacity to change.
In August 2020, CenterWatch reported that sites were feeling overwhelmed by growing administrative responsibilities. CenterWatch pointed to a survey indicating that about 80% of sites found that administrative responsibilities—such as managing study documents and regulatory file preparation—had increased “significantly” or “somewhat” over the preceding two years. Increased diversity in individual sponsors’ requirements, increased site responsibilities and increased protocol complexity topped the list of items most burdensome to sites.
Any given line item on a research professional’s task list in a protocol could include multiple steps, such as meetings, patient visits, labs and procedures, Beth Harper, chief learning officer at Pro-ficiency, noted. For instance, a protocol might call for patients to have two options—one on-site and one virtual—for some visits. That is convenient for patients, but that means that a site has to develop two pathways, along with the requisite training for both site staff and for patients.
The number of hours a site is putting into preparing for a study is the amount of time they are not working on that study, Jenna Rouse, chief experience officer at Pro-ficiency, said. Sponsors need to consider whether they would ask their own teams to do the same.
“The time taken to deal with these burdens is time that cannot be patient-facing or study-facing,” Scott Ballenger agreed. “I think it also weighs on the relationship with the sponsor and CRO, as well as contributing to site staff burnout.”
This is not a new problem. In a 2016 white paper, WCG pointed to use of multiple systems as a major source of overwork for clinical study teams. In the decade-plus preceding the white paper, biopharma companies began using individual clinical trial, regulatory, drug safety and learning management systems from a variety of vendors. These, in turn were customized to be more client-centric, which made it difficult for vendors to integrate their own products even within a single sponsor, much less across multiple companies and studies.
Specialized technology can also pose a burden. Ballenger noted that many a study comes with a unique suite of software applications, each of those requiring a learning curve. While some may be intuitive to use, others are frustrating and time-consuming.
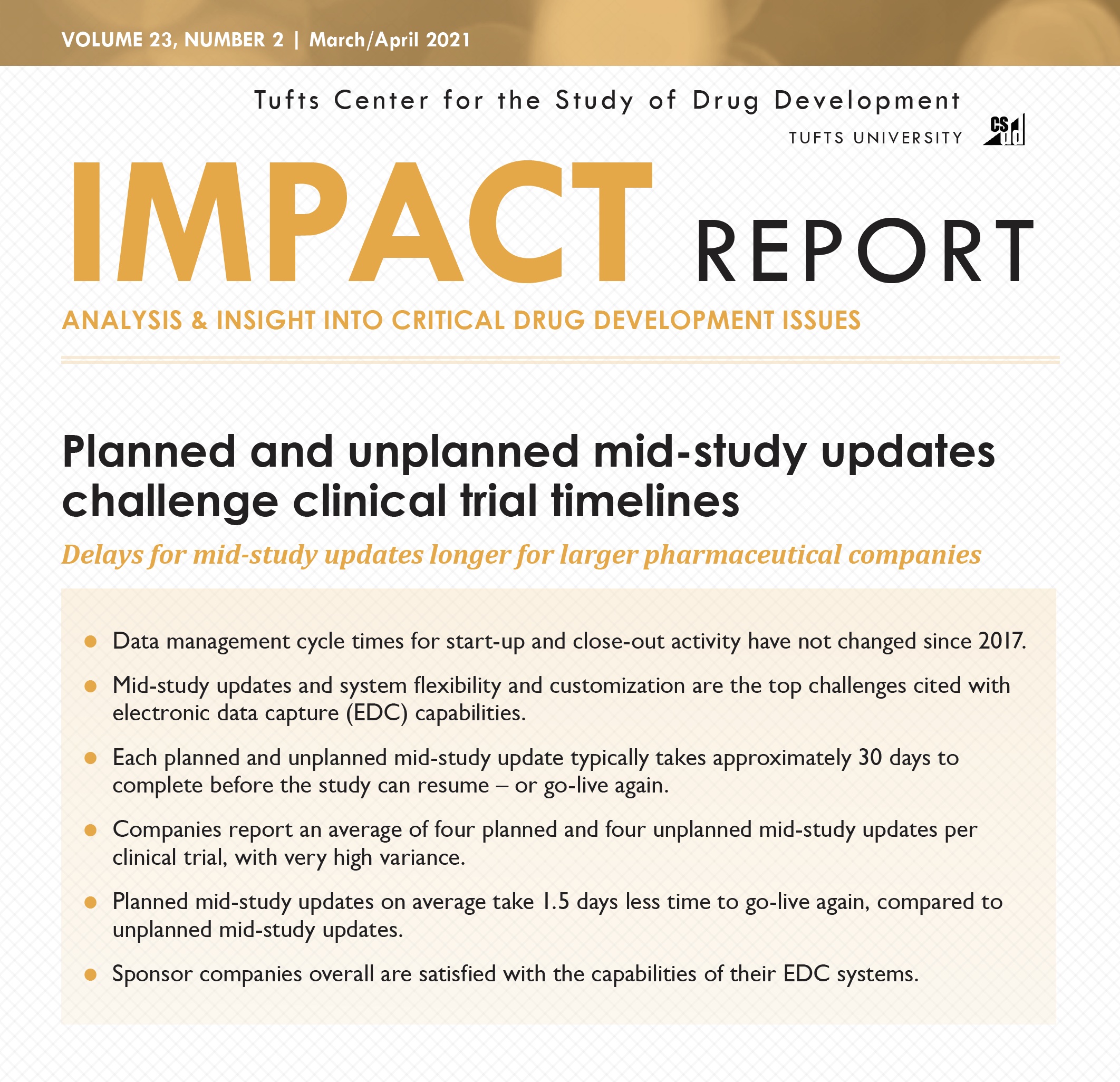
And not only are all these processes cumbersome and a drain on site professionals’ time, but they also up the possibility for errors or protocol deviations, which can add to the time and cost needed to complete a clinical trial. In its January/February 2022 Impact Report, Tufts Center for the Study of Drug Development (CSDD) reported that the number of protocol deviations and substantial amendments seen in clinical trials has increased in recent years.
“Deviations are a sign that something is not in accord with the protocol,” Rouse said. “If you train in a way that highlights areas where staff may not understand how their job is to be done in a specific trial, you can take action before deviations start costing sponsors money and research sites time for retraining.”
Targeted training holds answers
And training is one area in which sponsors can exercise a great deal of control over the time burdens they place on sites. Regulations require that sponsors provide appropriate training, so the safest position for pharma companies is to provide an immense amount of information on everything possible, Jeff Kingsley, CEO of Centricity Research, said. And when the information is both voluminous and irrelevant to a person’s job, staff are likely to tune it out.
GCP requirements, for instance, haven’t changed in decades. The content of the regulation remains the same, and has never included a mandated length of time for GCP certification to last, he said. But in order to check off all possible boxes, most sponsors mandate GCP certification—usually their own—for every individual trial.
This type of ‘spray and pray’ training—in which all staff get the same exhaustive training—doesn’t make sense and wastes clinical staff’s valuable time. Additionally, when research staff are inundated with masses of content irrelevant to their jobs, the information overload makes it more likely that they will forget content that is relevant.
But tailoring training to both the protocol and the people who need it not only will better assure a sponsor that each employee at a site is getting exactly the training they need, but it will save research staff the time burden of going through training they don’t need.
And the right training approach—one that helps identify areas of weakness or poor performance before a trial begins—will ensure that those that need extra help get it, while not forcing more proficient staff to sit through unnecessary training. This approach can also reduce protocol deviations, thus avoiding time- and money-sucking retraining after a study has begun.
Training should reflect the need to change or develop specific behaviors, Rouse explained. If a procedure or patient visit is to be done in a way that is different from the standard, staff will have to change familiar and ingrained behaviors. For example, when sites are trained in enrollment procedures for a given trial, they are expected to implement those procedures over time, sometimes with a considerable amount of lag time between receiving the training and enrolling patients. Training that lacks clear illustrations of important things like inclusion/exclusion criteria, visit timelines and schedules will be harder for staff to retain, Rouse said.
Sponsors need to consider whether the training they provide is focused enough on the specifics of the protocol. While some companies recognize that it’s not necessary to include standard-of-care, common procedures or well-known clinical practices, others take more of a cover-your-ass approach and include everything remotely relevant to the daily practices of a clinical trial.
A compromise approach for sponsors that want to be able to say they have covered every contingency could be to provide a written manual or slide deck for staff to use as a reference, but make the training more targeted, Rouse suggested.
Trainer, resources also important
Another consideration is who provides the training. This task is often given to CRAs, whose skills may not include effective teaching and commonly defaults to a mere re-reading of the protocol or rote presentation of PowerPoint slides that don’t address knowledge gaps at the research site.
“Someone reading the protocol is not useful,” Kingsley said. “We’ve already done that. Go into the science behind it and discuss what isn’t written in the protocol.”
Visualizations, flow charts and decision trees can help staff quickly understand the fine details of specific procedures than a half-day webinar or 200-page manual, Harper said, adding, “The goal of training should be to demystify the protocol and help site staff through the operational procedures.”
Kingsley added that sponsors should consider adult learning theory when developing training. For instance, training could have pieces aimed at people who learn best by reading, those who learn best visually and those who learn best by doing the activity. The 70-20-10 rule could also be useful, acknowledging that only 10% of adult learning comes from curriculum; 20% comes from mentorship and the remaining 70% from the capacity to connect with others on how best to accomplish tasks and goals.
He also advocated use of online communities where research site staff can pose questions to and have discussions with others working in the same areas or on the same protocol.
And it’s important that sponsors not assume what sites need in terms of training. Sites should be selected because of their general clinical trial skills, so training should focus tightly on the protocol, Rouse said. One way this could be achieved is by getting input from sites on what training they need to ensure thorough understanding of the protocol.
This approach to training does require an upfront investment. But when enrollment lags or deviations occur due to training failure, sponsors will have to take the time, effort and cost to retrain staff anyway. And retraining further adds to the time burden on research staff.
Standardization sought, industry solutions few
Standardization of boilerplate training that applies to most clinical trials—ideally provided by an independent third party rather than a sponsor—would go a long way toward reducing training-related burdens on research staff, Kingsley said.
Training redundancy can act as a huge time sink for research sites. Some industry efforts have been made to reduce redundancies. Transcelerate, for instance, has aimed to reduce inefficiencies through efforts like a shared investigator platform to streamline certain boilerplate activities like general GCP training. The idea is that if researchers at a site are certified through a Transcelerate partner GCP course, that certification would be accepted by other partners.
“A lot of times, anything in the training that is not protocol-specific is going to lead to redundancy,” Rouse said. “The simplest thing is to see if there is a standard version of the training you want to deliver—such as EUCTR, informed consent, or GCP—and tap into that to relieve redundancy burdens on sites. An hour of a site’s time is worth saving; it is better for them to spend that time on finding the right trial participant than doing more routine certification.”
Kingsley also pointed to retraining related to protocol amendments as an unnecessary burden. Many protocol amendments are narrow in scope and irrelevant to many staff. For instance, an amendment that affects how labs operate still leads to the entire study staff having to take time to undergo the retraining. It would be better to focus amendment-related training to only the staff that would be affected by the change, he said.
“But redundancy is not necessary,” Rouse said. “Anytime a sponsor can choose a central GCP or other program as a standard, that will reduce the burden on sites.”
The ACRP also provides a GCP training program, including a simulation approach launched last year, with an eye toward a standardized approach that reduces the number of times sites have to complete GCP certification.
And WCG offers a survey designed to help sponsors determine how much of a burden their study would place on a site based on protocol and operational complexity.
However, it’s unclear how much traction this type of project can gain, as many sponsors want to use their own courses.
But sponsors should begin to view research site staff as high-value customers as a first step to addressing these burdens, Ballenger suggested. That means examining all processes and requirements to find ways to reduce friction and support the site. For instance, in terms of training, a stack of PowerPoint slides is unlikely to be appealing to most sites; sponsors should look at ways to signal that they care about the site’s learning experience.
To learn more about a training approach that is tailored to the needs of users and sites, visit http://proficiency1.wpenginepowered.com/simulation-training
Dave Hadden is an entrepreneur and technology innovator, founding Pro-ficiency and pioneering the fields of A.I.-based medical decision-support, Training Analytics, and Virtual Patient Simulation (VPS). Dave has focused his passion for technological innovation and learning systems in the field of clinical trials, helping sponsors make their studies more accurate and efficient through finding the right technology mix such as virtualization, performance management and applied behavioral sciences to produce the most effective, lasting, and engaging results for clinical trials.











{kind=link}
{kind=link}